الانف والأذن
Acute Otitis Externa
“last update: 28 April 2024” Download Guideline
– Executive Summary
This Guideline is intended to provides evidence-based recommendations to manage acute otitis externa (AOE), defined as diffuse inflammation of the external ear canal, which may also involve the pinna or tympanic membrane. The variations in management of AOE and the importance of accurate diagnosis suggest a need for applying the clinical practice guideline. The primary outcome considered
in this guideline is clinical resolution of AOE
◾ Clinicians should distinguish diffuse acute otitis externa (AOE) from other causes of otalgia, otorrhea, and inflammation of the external ear canal.
◾ Clinicians should assess the patient with diffuse AOE for factors that modify management (nonintact tympanic membrane, tympanostomy tube, diabetes, immunocompromised state, priorradiotherapy).
◾ The clinician should assess patients with AOE for pain and recommend analgesic treatment based on the severity of pain.
◾ Clinicians should not prescribe systemic antimicrobials as initial therapy for diffuse, uncomplicated AOE unless there is extension outside the ear canal or the presence of specific host factors that would indicate a need for systemic therapy.
◾ Clinicians should use topical preparations for initial therapy of diffuse, uncomplicated AOE.
◾ Clinicians should inform patients how to administer topical drops and should enhance delivery of topical drops when the ear canal is obstructed by performing aural toilet, placing a wick, or both.
◾ When the patient has a known or suspected perforation of the tympanic membrane, including a tympanostomy tube, the clinician should recommend a non-ototoxic topical preparation.
◾ If the patient fails to respond to the initial therapeutic option within 48 to 72 hours, the clinician should reassess the patient to confirm the diagnosis of diffuse AOE and to exclude other causes of illness.
Acute Rhinosinusitis
“last update: 5 August 2024” Download Guideline
– Executive Summary
1- Definition: Acute rhinosinusitis (ARS) is considered when symptoms and signs are present less than 4 weeks. (Strong recommendation)
2- Diagnosis of acute ARS through symptoms/signs and duration:
-Symptoms must include most of the followings (All can be included in CPODS)
C: Congestion, P: Pain, O: Obstruction,D: Drainage/Discharge,S: Smell affection
(Strong recommendation)
3- A thorough physical examination that includes inspection , palpation of the maxillary and frontal sinus, as well as anterior rhinoscopy (evidence of inflammation, mucosal oedema, and discharge). (Conditional recommendation)
4- Objective evidence of ARS on nasal endoscopy, antral puncture, or radiographic imaging (X-ray, ultrasonography, or CT) is not required for the diagnosis in uncomplicated cases. (Strong recommendation against)
5- ESR and CRP are inflammatory markers found to be elevated during ARS, but they are not routinely used for diagnosis because of their limited specificity. It can be used in COVID-19 . (Conditional recommendation)
6- Differentiate viral from bacterial ARS: -Duration is thought to be a key factor differentiating ABRS from AVR, with persistence of symptoms beyond 7-10 days or worsening of symptoms after 5 days being indicators of development of post-viral ABRS.
-Clinical factors associated with symptoms and signs ABRS include:
Timing of the disease, worsening of the disease, purulent nasal discharge on rhinoscopy, localized unilateral pain, severe pain over the teeth and maxilla, and fever > 38˚C. (conditional recommendation)
7- Consider initial watchful waiting in uncomplicated cases with assurance of follow up. (conditional recommendation)
8- Institution of antibiotic therapy if:
A. No improvement after 4-7 days or worsening at any time,
B. Mitigating circumstances with drug resistance e.g., severe symptoms and immunocompromised states
C. Concern for impending complications
D. Suspected odontogenic source
E. Prior antibiotics (1 month), prior hospitalization (5 days) and comorbidities.
(Conditional recommendation)
9- If a decision is made to treat ABRS with an antibiotic, the clinician should prescribe amoxicillin with clavulanate (conditional recommendation)
10- First time non-responders can be based on lack of clinical improvement following treatment within 5 days in adults and 3 days in children. -Use second line antimicrobial agents. (Conditional recommendation)
11- In patients with ABRS suspected to have suppurative complications, axial, coronal and sagittal views with contrast-enhanced computed tomography (CT) is recommended. (Conditional recommendation)
12- Recurrent acute rhinosinusitis RARS is diagnosed when At least 4 attacks of ABRS/year are documented (Conditional recommendation)
-Consider Nasal endoscopy and/or CT imaging are an option during at least one episode of suspected RARS (Conditional recommendation)
-Endoscopic sinus surgery (ESS) is recommended for patients with RARS. (Conditional recommendation)
Allergic rhinitis
“last update: 28 April 2024” Download Guideline
– Executive Summary
▪️ PATIENT HISTORY AND PHYSICAL EXAMINATION: Clinicians should make the clinical diagnosis of AR when patients present with a history and physical examination consistent with an allergic cause and 1 or more of the following symptoms: nasal congestion, runny nose, itchy nose, or sneezing. Findings of AR consistent with an allergic cause include, but are not limited to, clear rhinorrhea, nasal congestion, pale discoloration of the nasal mucosa, and red and watery eyes.
▪️ ALLERGIC TESTING: Clinicians should perform and interpret, or refer to a clinician who can perform and interpret, specific IgE (skin or blood) allergy testing for patients with a clinical diagnosis of AR who do not respond to empiric treatment, or when the diagnosis is uncertain, or when knowledge of the specific causative allergen is needed to target therapy.
▪️ IMAGING: Clinicians should not routinely perform sinonasal imaging in patients presenting with symptoms consistent with a diagnosis of AR.
▪️ ENVIRONMENTAL FACTORS: Clinicians may advise avoidance of known allergens or may advise environmental controls in AR patients who have identified allergens that correlate with clinical symptoms.
▪️ CHRONIC CONDITIONS AND COMORBIDITIES: Clinicians should assess patients with a clinical diagnosis of AR for, and document in the medical record, the presence of associated conditions such as asthma, atopic dermatitis, sleep-disordered breathing, conjunctivitis, rhinosinusitis, and otitis media.
▪️ PHARMACOLOGIC THERAPY:
A- TOPICAL STEROIDS: Clinicians should recommend intranasal steroids for patients with a clinical diagnosis of AR whose symptoms affect their quality of life.
B- ORAL ANTIHISTAMINES: Clinicians should recommend oral second-generation/less sedating antihistamines for patients with AR and primary complaints of sneezing and itching.
C- INTRANASAL ANTIHISTAMINES: Clinicians may offer intranasal antihistamines for patients with seasonal, perennial, or episodic AR.
D- ORAL LEUKOTRIENE RECEPTOR ANTAGONISTS (LTRAs): Clinicians should not offer LTRAs as primary therapy for patients with AR.
E- SALINE NASAL WASH: Saline nasal wash is recommended as part of the treatment strategy for AR.
F- ORAL CORTICOSTEROIDS: Recommendation against the routine use of oral corticosteroids for AR.
G- CROMOLYN: Disodium chromoglycate (DSCG) may be considered for the treatment of AR, particularly in patients known triggers and who cannot tolerate INCSs.
H- INTRANASAL ANTICHOLINERGIC: Ipratropium bromide nasal spray may be considered as an adjunct medication to INCSs in PAR patients with uncontrolled rhinorrhea.
I- OMALIZUMAB: Strong recommendation against use in treatment of allergic rhinitis alone
▪️ COMBINATION THERAPY: Clinicians may offer combination pharmacologic therapy in patients with AR who have inadequate response to pharmacologic monotherapy.
▪️ PHARMACOLOGIC THERAPY OF ALLERGIC RHINITIS ASSOCIATED WITH BRONCHIAL ASTHMA:
✔️ Use of systemic corticosteroid is not recommended for routine use in AR with comorbid asthma.
✔️ Omalizumab: Recommended for those patients with clear IgE-mediated allergic asthma with coexistent AR who fail conventional therapy.
▪️ IMMUNOTHERAPY: Clinicians should offer, or refer to a clinician who can offer, immunotherapy (sublingual or subcutaneous) for patients with AR who have inadequate response to symptoms with pharmacologic therapy.
▪️ INFERIOR TURBINATE REDUCTION: Clinicians may offer, or refer to a surgeon who can offer, inferior turbinate reduction in patients with AR with nasal airway obstruction and enlarged inferior turbinates who have failed medical management.
▪️ HERBAL THERAPY: No recommendation regarding the use of herbal therapy for patients with AR.
AUDIOLOGY Tinnitus
“last update: 19 May 2024” Download Guideline
– Executive Summary
Auditory Brainstem Response (ABR) Testing in Babies
“last update: 26 August 2024” Download Guideline
– Executive Summary
Effective and consistent hearing measurement in babies is important for early intervention.
Of particular importance are guidelines to unify testing, data reporting particularly as universal hearing screening is being implemented in EGYPT
● Choice of electrodes & application Skin should be gently abraded. Appropriate options include abrasive electrode paste and cleaning stick with soft cotton material. Single use disposable electrodes are recommended. (Strong recommendation).
● Sedation is not necessary in babies under 12 weeks of age and should be used in babies under 12 months of age only in exceptional circumstances. Sleep deprivation, feeding and diaper change in most situations will lead to natural sleep and lessen activity. (Strong recommendation)
● In order to achieve frequency specificity, thresholds should be measured for at least two frequency audiometric regions:
1. Low frequency thresholds using 0.5 kHz tone bursts or tone pips .
2. High frequency thresholds using 2 or 4 kHz TP / TB or clicks. (Strong recommendation)
● Definition of ABR threshold It is defined (BSA, NHSP 2013) as the lowest level at which a clear response (CR) is present, with a response absent (RA) 5 – 10dB below threshold, under good recording conditions.
● Criteria for ABR response & threshold:
1-Reproducibilty of at least two response traces: visual and graphic.
2-Reproducibility of responses for all intensity i/o functions.
3-Threshold is the reproducible response at the lowest stimulus intensity reached.
(Strong recommendation)
● Calibration :
1. Subjective stage A listening check using 50/sec RR.
2. Reference equivalent SPL for clicks and tone pips if and when feasible.
3. Psychoacoustic calibration control is feasible and easy and can be routinely done.
(Conditional recommendation)
● Reporting:
Results should be clearly marked using the symbols ‘=’, ‘≤’ or ‘<=’, and ‘>’ in addition to the descriptive statements, when important rehabilitation decisions are made.
(Conditional Recommendation)
Articulation Disorders (Speech Sound Disorders)
“last update: 29 August 2024” Download Guideline
– Executive Summary
1. How to identify speech sound disorders from organic causes of impaired speech production:
a. History taking: to exclude delayed developmental milestones, sensori-neural hearing loss, cleft palate, and dysarthria. (strong recommendation)
b. Thorough general and otolaryngological examination. (strong recommendation)
2. Speech sound assessment: formal language and articulation tests to assess language and phonology, followed by:
a. Phonetic transcription for the phonological errors and any special context where they occur. (strong recommendation)
b. Identify error pattern: omission, substitution, or distortion. (strong recommendation)
c. Stimulability. (strong recommendation)
d. Intelligibility. (strong recommendation)
3. Treatment options:
a. Contextual therapy: this approach utilizes that speech sounds are produced in syllable- based contexts in connected speech and some phonemic/phonetic contexts can facilitate correct production of a particular sound. (conditional recommendation)
b. Contrast therapy: minimal opposition, maximal opposition, or multiple opposition therapy. (strong recommendation)
c. Cycle approach: the child is provided with a practice on a given target for a predetermined period, before moving to another target for a predetermined period, and then cycles again. (strong recommendation)
d. Metaphone therapy: bringing about phonological change through increasing the metalinguistic awareness. (conditional recommendation)
e. Naturalistic intelligibility intervention: naturalistic intervention refers to the notion that phonological disorders should be corrected in communication situations that resemble everyday life. (strong recommendation)
Benign paroxysmal positional vertigo (ECPG)
“last update: 27 August 2024” Download Guideline
– Executive Summary
Clinicians should diagnose posterior semicircular canal BPPV when vertigo associated with torsional, up beating nystagmus is provoked by the Dix-Hall pike maneuver, performed by bringing the patient from an upright to supine position with the head turned 45° to one side and neck extended 20° with the affected ear down. The maneuver should be repeated with the opposite ear down if the initial maneuver is negative. (Strong recommendation)
If the patient has a history compatible with BPPV and the Dix-Hallpike test exhibits horizontal or no nystagmus, the clinician should perform, or refer to a clinician who can perform, a supine roll test to assess for lateral semicircular canal BPPV. (Strong recommendation)
Clinicians should differentiate, or refer to a clinician who can differentiate, BPPV from other causes of imbalance, dizziness, and vertigo. (Strong recommendation)
Clinicians should assess patients with BPPV for factors that modify management, by the recommended repositioning maneuvers, including impaired mobility or balance, central nervous system disorders, a lack of home support, and/or increased risk for falling. (Strong recommendation)
Clinicians should not obtain radiographic imaging in a patient who meets diagnostic criteria for BPPV. (Strong recommendation against)
Clinicians should not order laboratory vestibular testing in a patient who meets diagnostic criteria for BPPV in the absence of additional vestibular signs and/or symptoms inconsistent with BPPV that warrant testing. Vestibular testing may be ordered in case of recurrence, persistence of complaint after repositioning manoeuvre or in the presence of atypical nystagmus (Conditional recommendation against)
Clinicians should treat, or refer to a clinician who can treat, patients with posterior canal BPPV with a canalith repositioning procedure. Epley’s or Semont’s are equivocally effective for posterior canal BPPV. Semont’s is recommended in cupulolithiasis than Epley’s. (Strong recommendation)
The barbecue roll manoeuvre or Gufoni manoeuvre appear moderately effective for the geotropic form of lateral semi-circular canal BPPV. (Conditional recommendation)
Clinicians may not routinely recommend post procedural postural restrictions after canalith repositioning procedure for posterior canal BPPV. Post procedural postrural restriction might be recommended in selected cases as in failure (or repeated failure) of the repositioning maneuvers, recurrent cases, or cases associated with other vestibular pathology as MD or vestibular Migraine. (Conditional recommendation against)
1-2 sessions would resolve the condition in 87-100% of patients. A minority would require a 3ed trial. Otherwise persistent BPPV is suspected. (Strong recommendation)
Clinicians should start with CRP (or modified) even in those patients who are very obese; have severe cervical or lumber discs; or upon patient’s preference. In the latter case patients should be instructed to avoid activities that may increase the risk of falls until symptoms resolve. (Strong recommendation)
Clinicians may offer observation with follow up only if there is difficulty in performing successful manoeuvre after trials in some patients as : very obese; severe cervical or lumber discs; or upon patient’s preference not to repeat the manoeuvre. (Strong recommendation)
VR should be considered an option in the treatment of BPPV rather than a recommended first-line treatment modality. Home based Brandt-Daroff exercises is indicated in patients with persistent dizziness or imbalance after successful CRP or patients who refuse CRP.A more comprehensive customized VR program is indicated in patients with other vestibular pathology or with comorbid impairments that require balance rehabilitation specially in elderly. (Strong recommendation)
Clinicians should not treat BPPV with vestibular suppressant medications such as antihistamines and/ or benzodiazepines. Exceptions: Prior to CRP in patients with severe nausea and/or vomiting, or patients previously manifested severe nausea and/or vomiting during testing. (Strong recommendation against)
Clinicians should reassess patients within an initial period of observation following the canalith repositioning procedure (40 minutes up to one week) to document resolution, need for repetition of CRP session or persistence of symptoms. (Strong recommendation)
Clinicians should evaluate, or refer to a clinician who can evaluate, patients with persistent symptoms for unresolved BPPV and/or underlying peripheral vestibular or central nervous system disorders. (Strong recommendation)
Clinicians should educate patients regarding the impact of BPPV on their safety, the potential for disease recurrence, and the importance of follow-up. (Strong recommendation)
Cerebrospinal fluid rhinorrhea (ECPG)
“last update: 10 June 2024” Download Guideline
– Executive Summary
Traumatic and iatrogenic CSF leaks
Consideration for nonsurgical management within the first 7 days is feasible in traumatic skull base injuries (strong recommendation)
Lumbar drains may shorten the interval to traumatic CSF leak cessation during conservative management (conditional recommendation)
The evidence for acetazolamide in traumatic or iatrogenic CSF leaks is lacking (strong recommendation).
There is a lack of evidence to support prophylactic antibiotics administration in patients with a traumatic CSF leak (conditional recommendation).
For defects in the ethmoid roof and sphenoid, Non-iatrogenic (after conservative measures fail) and iatrogenic traumatic CSF (generally not treated conservatively) leaks can be repaired endoscopically with high success rates (strong recommendation)
For frontal sinus defects, the transnasal endoscopic approach to frontal sinus CSF leaks is safe and effective in select patients, but may have higher rates of failure than other locations (strong recommendation).
Spontaneous CSF rhinorrhea
There is a direct relationship between spontaneous CSF leaks and IIH; most spontaneous leaks represent a variant of IIH (strong recommendation).
After clinical examination, B2- transferrin and beta trace protein are the initial preferred methods of detection of CSF leaks (conditional recommendation).
For site of leak detection, High resolution CT (HRCT) and Magnetic resonance imaging (MRI) are the initial imaging modalities (non invasive). CT cysternography with intrathecal dye injection (Invasive) may be required if the previous measures failed to determine the site of leak (conditional recommendation).
Perioperative lumbar drains are not necessary for the successful repair of most spontaneous CSF leaks. Lumbar drains remain an option for adjunctive measures such as administration of intrathecal fluorescein or high-risk cases (strong recommendation) (Recommendation against except in high risk cases).
Postoperative ICP management should be considered in patients with spontaneous CSF leaks and elevated ICPs. Acetazolamide can be used as an effective ICP-lowering medication with an option of CSF shunting procedures in patients unable to tolerate medical management or with recalcitrantly elevated ICPs or recurrent CSF leaks (conditional recommendation).
Reconstructive technique should be left to the discretion of the surgeon with consideration of defect location, size and etiology (strong recommendation).
Intrathecal application is an off-label use of fluorescein for which informed consent must be obtained from the patient (conditional recommendation).
Cochlear Implantation: Phoniatric perspective
“last update: 27 August 2024” Download Guideline
– Executive Summary
The goals of cochlear implantation in children are acquiring normal speech and language development, achieving higher levels academically, enrolling in main streaming and developing better sense of security and better quality of life (Strong recommendation).
As for adult recipients of CI, main goals are improved social and work quality of life, with less stressful events (Strong recommendation).
– Duration of deafness, hearing aid use prior to implantation, and age at implantation, can affect candidacy and predict post-operative outcomes (Strong recommendation).
– Pre lingually deafened adolescents and adults may benefit from cochlear implantation and should not be excluded from candidacy (Conditional recommendation).
– Children with disabilities in addition to deafness may benefit from cochlear implantation in quality-of-life outcomes and environmental awareness. These groups should not be excluded from candidacy. Families should be counseled regarding realistic expectations (Strong recommendation).
– A speech and language evaluation may be recommended in adult candidacy evaluations and could be considered critical in pediatric candidacy evaluations (Strong recommendation).
– High performance in children who use a cochlear implant has been linked to full-time use of the cochlear implant in home and school environments (Strong recommendation).
– The amount and quality of language used by parents/caregivers of children who use cochlear implants has a strong influence on these children’s linguistic development. (Strong recommendation).
– Bilateral stimulation should be considered for all individuals who use a cochlear implant, if not otherwise contraindicated.
Clinicians should be able to:
-Work in a multidisciplinary team of related specialties to ensure proper candidate selection and successful outcomes post implantation.
– Acquire full history from the patient/caregiver.
– Perform evaluation of the preimplant auditory skills, speech, language and voice evaluation.
– Implement different strategies of auditory training to enhance auditory skills development in order to acquire normal spoken receptive and expressive language development (Strong recommendation).
All clinicians should be aware and informed to consider the following:
• Red Flags that need any referral for Assessment/ Management must be taken into consideration.
• Why and when to refer to other specialties .
• Management should be targeted towards implementation of proper auditory training for acquisition of spoken language skills, aiming to decrease the gap between the chronological age and the language age (Strong recommendation).
Deep Neck Space Infections (DNSIs)
“last update: 5 August 2024” Download Guideline
– Executive Summary
Dysarthria (ECPG)
“last update: 19 May 2024” Download Guideline
– Executive Summary
The scope of the guidelines in the diagnosis and management of Dysarthria
1. Any subject with speech difficulty should undergo:
a). History taking ( strong recommendation)
b). Auditory perceptual assessment (APA) (strong recommendation)
c). Examination that includes both neurological examination and ENT examination ( strong recommendation)
2. By the end of this assessment battery, dysarthria by its type and severity should be diagnosed with exclusion of other speech disorders. ( conditional recommendation )
3. Rehabilitation will start tailoring a therapeutic plan that may include all the aspects (in blue rectangles) or some of them according to the most prominent speech parameters affecting the speech intelligibility of the patient.(strong recommendation)
4. For every aspect, your therapeutic trials may succeed or fail, and accordingly measurement of the outcome is of value every three months. Work with the patient in more than one aspect at the same time and not one of them at a time.( conditional recommendation)
5. Resonance therapy through training ,however, if failed shift to obturator.( conditional recommendation)
6. Articulation, respiration, phonation and prosody have many techniques to correct them.(conditional recommendation)
7. Prognosis and therapy termination is determined when patient’s satisfaction is reached and when the Auditory perceptual assessment showed correction and elimination of difficulties. (conditional recommendation)
8. Augmentative and alternative communication methods should be considered in case achieved progress is unsatisfactory, particularly in patients having severe difficulties. (strong recommendation )
Early & Late Laryngeal Cancer (ECPG)
“last update: 10 June 2024” Download Guideline
– Executive Summary
Hoarseness (Dysphonia)
“last update: 28 April 2024” Download Guideline
– Executive summary
This guideline provides evidence-based recommendations on managing hoarseness (dysphonia) which affects nearly one-third of the population at some point in their lives. This guideline applies to all age groups evaluated in a setting where hoarseness would be identified or managed. It is intended for all clinicians who are likely to diagnose and manage patients with hoarseness.
· The clinician should not routinely prescribe antibiotics to treat hoarseness.
· The clinician should advocate voice therapy for patients diagnosed with hoarseness that reduces voice-related QOL.
· The clinician should diagnose hoarseness (dysphonia) in a patient with altered voice quality, pitch, loudness, or vocal effort that impairs communication or reduces voice-related QOL.
· The clinician should assess the patient with hoarseness by history and/or physical examination for factors that modify management, such as one or more of the following: recent surgical procedures involving the neck or affecting the recurrent laryngeal nerve, recent endotracheal intubation, radiation treatment to the neck, a history of tobacco abuse, and occupation as a singer or vocal performer.
· The clinician should visualize the patient’s larynx or refer the patient to a clinician who can visualize the larynx, when hoarseness fails to resolve by a maximum of three months after onset, or irrespective of duration if a serious underlying cause is suspected.
· The clinician should not obtain computed tomography or magnetic resonance imaging of the patient with a primary complaint of hoarseness prior to visualizing the larynx.
· The clinician should not prescribe anti reflux medications for patients with hoarseness without signs or symptoms of gastroesophageal reflux disease.
· The clinician should not routinely prescribe oral corticosteroids to treat hoarseness.
· The clinician should visualize the larynx before prescribing voice therapy and document/communicate the results to the speech-language pathologist.
· The clinician should prescribe or refer the patient to a clinician who can prescribe, botulinum toxin injections for the treatment of hoarseness caused by adductor spasmodic dysphonia.
· The clinician may perform laryngoscopy at any time in a patient with hoarseness or may refer the patient to a clinician who can visualize the larynx.
· The clinician may educate/counsel patients with hoarseness about control/preventive measures.
Otitis Media with Effusion
“last update: 28 April 2024” Download Guideline
– Executive Summary
This Guideline is concerned with diagnosis and treatment decision of otitis media with effusion. This is targeting a child aged 2 months through 12 years with OME, with or without developmental disabilities or underlying conditions that predispose to OME and its sequelae. This patient characteristics correspond with inclusion criteria in many OME studies. This guideline, however, does not apply to patients <2 months or >12 years of age.
· The clinician should document the presence of middle ear effusion with pneumatic otoscopy when diagnosing OME in a child.
· The clinician should perform pneumatic otoscopy to assess for OME in a child with otalgia, hearing loss, or both.
· The clinician should obtain tympanometry in children with suspected OME for whom the diagnosis is uncertain after performing (or attempting) pneumatic otoscopy.
· The clinician should manage the child with OME who is not at risk with watchful waiting for 3 months from the date of effusion onset (if known) or 3 months from the date of diagnosis (if onset is unknown).
· The clinician may recommend Autoinflation using a balloon more than 3 times a day as a treatment option.
· The clinician should recommend against (catheterization) as it can result in TM perforation and affect the surrounding organs (epistaxis, emphysema, etc.).
· The clinician should recommend against using intranasal or systemic steroids for treating OME.
· The clinician should recommend against using systemic antibiotics for treating OME, and should recommend against using antihistamines, decongestants, or both for treating OME.
· The clinician should document in the medical record counseling of parents of infants with OME who fail a newborn screening regarding the importance of follow-up to ensure that hearing is normal when OME resolves and to exclude an underlying sensorineural hearing loss.
· The clinician should determine if a child with OME is at increased risk for speech, language, or learning problems from middle ear effusion because of baseline sensory, physical, cognitive, or behavioral factors.
· The clinician should evaluate at-risk children for OME at the time of diagnosis of an at-risk condition and at 12 to 18 months of age (if diagnosed as being at risk prior to this time).
· The clinician should not routinely screen children for OME who are not at risk and do not have symptoms that may be attributable to OME, such as hearing difficulties, balance (vestibular) problems, poor school performance, behavioral problems, or ear discomfort.
· The clinician should educate children with OME and their families regarding the natural history of OME, need for follow-up, and the possible sequelae.
· The clinician should obtain an age-appropriate hearing test if OME persists for 3 months or longer OR for OME of any duration in an at-risk child.
· The clinician should counsel families of children with bilateral OME and documented hearing loss about the potential impact on speech and language development.
· The clinician should reevaluate, at 3- to 6-month intervals, children with chronic OME until the effusion is no longer present, significant hearing loss is identified, or structural abnormalities of the eardrum or middle ear are suspected.
· The clinician should recommend tympanostomy tubes when surgery is performed for OME in a child <4 years old; adenoidectomy should not be performed unless a distinct indication exists (nasal obstruction, chronic adenoiditis).
· The clinician should recommend tympanostomy tubes, adenoidectomy, or both when surgery is performed for OME in a child ³4 years old.
· The clinician should not place long-term tubes as initial surgery for children who meet the criteria for tube insertion unless there is a specific reason based on an anticipated need for prolonged middle ear ventilation beyond that of a short-term tube.
· The clinician should not routinely prescribe postoperative antibiotic ear drops after tympanostomy tube placement.
· The clinician should prescribe topical antibiotic ear drops only, without oral antibiotics, for children with uncomplicated acute tympanostomy tube otorrhea.
· The clinician should not encourage routine, prophylactic water precautions (use of earplugs or headbands, avoidance of swimming or water sports) for children with tympanostomy tubes.
· The clinician should document resolution of OME, improved hearing, or improved quality of life when managing a child with OME.
Otology
“last update: 28 April 2024” Download Guideline
– Executive Summary
|
|
Chief Editor: Reda Kamel1 General Secretary: Ahmed Ragab2 General Coordinator: Baliegh Hamdy3 Scientific Board: Ashraf Khaled,4 Mohamed Ghonaim,5 Mahmoud Abdel Aziz,6 Tarek Ghanoum,7 Mahmoud Yousef8 Otology Chief Manager: Ali Mahrous12 Assembly board: Sherif Guindi,9 Yasser Shewel,10 Mahmoud Mandour,6 Usama Kamal,11 Ahmed Hesham Galal10 Grading Board (In alphabetical order): Mohamed Abdel Badie,5 Gamal Abdel Fattah,1 Doaa Abdel Halim,12 Ashraf Alhamshary,13 Mahmoud Badr El-Dine,10 Aziz Belal,10 Ezz Eldine Elshikh,14 Fathi Erfan,6 Ayman Fouad,6 Amr Galal,15 Mahmoud Ahmad Hamed,16 Haytham Hassan,10 Nabila Ibrahim,12 Ashraf Lotfy,17 Osama Metwaly,1 Amir Gorguy Mina,10 Waleed Monir,5 Ihab Nada,18 Mahmoud Qotb,9 Mohamed Refaat,19 Ashraf Salah el Dine,17 Yousef Shabana6 Reviewing Board (In alphabetical order): Hani Garem,10 Hisham Hamad,6 Saad El Zayat15 Hesham Taha20 Iman Iskandar21 Lydia Youssef22 Ministry of health ECPG steering committee: Reda Kamel1, Ahmed Ragab2, Mahmoud Abdelaziz6, Mohamed Elsheikh6, Sherif Guindi9, Ali Mahrous12, Louay Sharkawy1, Saad Elzayat15, Ahmed Abu Elwafa23, Iman Sadek20, Mahmoud Yousef8, Samir Halim24, Ahmed Mustafa25, Ehab Seifein 25, Ashraf Lotfy26, Mohamed Eltokhy27, Tamer Azzam27 1Otorhinolaryngology Dep. Faculty of Medicine/Cairo University, 2Otorhinolaryngology Dep. Faculty of Medicine/Menoufia University, 3Otorhinolaryngology Dep. Faculty of Medicine/Minia University, 4Otorhinolaryngology Dep. Faculty of Medicine/Beni-Suef University, 5Otorhinolaryngology Dep. Faculty of Medicine/Mansoura University, 6Otorhinolaryngology Dep. Faculty of Medicine/Tanta University, 7Audiovestibular Unit, Otorhinolaryngology Dep. Faculty of Medicine/Cairo University, 8Phoniatrics Unit, Otorhinolaryngology Dep. Faculty of Medicine/Ain Shams University, 9Otorhinolaryngology Dep. Faculty of Medicine/Fayoum University, 10Otorhinolaryngology Dep. Faculty of Medicine/Alexandria University, 11Otorhinolaryngology Dep. Faculty of Medicine/South Valley University, 12Otorhinolaryngology Dep. Faculty of Medicine/Al Azhar University, 13Otorhinolaryngology Dep. Faculty of Medicine/Banha University, 14Otorhinolaryngology Dep. Faculty of Medicine/Zagazig University, 15Otorhinolaryngology Dep. Faculty of Medicine/Kafr El Shiekh University, 16Otorhinolaryngology Dep. Faculty of Medicine/Sohag University, 17Otorhinolaryngology Dep. Faculty of Medicine/Military Medical Academy, 18Otorhinolaryngology Dep. Faculty of Medicine/Misr University for Science and Technology, 19Otorhinolaryngology Dep. Faculty of Medicine/Suez Canal University Faculty of Medicine/Al Azhar University, 20Audiovestibular Unit, Otorhinolaryngology Department, Faculty of Medicine/ Ain Shams University, 21Paediatric Dep. Faculty of Medicine/Cairo University, 22Head nurse, Out-patient Clinic, Hayat Medical Center (HMC), 23 Otorhinolaryngology Department, Faculty of Medicine/ Assiut University, 24Otorhinolaryngology Department Mataria Teaching Hospital, 25Otorhinolaryngology Department, Faculty of Medicine/ Hearing and Speech Institute, 26Otorhinolaryngology Department Secretariat of the Ministry of Defense, 27Otorhinolaryngology Department Ministry of Interior Medical Services Sector. – Sincere thanks extend to the secretaries: Samar Hussein and Eman Ragab, as well as the editor: Mohamed Salah |
Abbreviations
|
|
AAP American academy of pediatricians AAFP American academy of family practitioners AOM Acute otitis media CPG Clinical Practice Guideline GRADE Grading of Recommendations Assessment, Development and evaluation MEE Middle ear effusion MRI Magnetic Resonance Imaging OME Otitis media with effusion RCT Randomized controlled trial TM Tympanic membrane |
PHONIATRICS Brain damage motor handicap BDMH CORRECTED
“last update: 10 June 2024” Download Guideline
– Executive Summary
1- Assessment of the child with BDMH (CP):
A. Elementary diagnostic procedures:
Through history taking and clinical examination (including vocal tract and neurological examination):
◽ Exclude progressive neurological disorders such as neurodegenerative diseases.
◽ Exclude non-specific motoric insults causing diffuse brain damage (global developmental delay/intellectual disability).
◽ Establish the presence of specific motoric insult.
◽ Determine the type of BDMH (CP) whether spastic, ataxic, dyskinetic, or atonic. (Strong recommendation)
B. Clinical diagnostic aids: including
◽ Psychometric evaluation to determine IQ, mental age, and social age.
◽ Language assessment by standardized Arabic language test to determine receptive, expressive, and total language ages.
◽ Speech assessment for associated dysarthria.
◽ Swallowing assessment for associated feeding and swallowing disorders including instrumental evaluation if needed. (Strong recommendation)
C. Additional instrumental measures: including
◽ Magnetic resonance imaging (MRI): to investigate etiology in a child or young person with suspected or known BDMH if this is not clear from history or clinical examination.
◽ Audiometry: Initial baseline and regular ongoing hearing assessment are necessary.
◽ Electroencephalogram (EEG): Since epilepsy occurs in around 1 in 3 children with BDMH (CP).
◽ Ophthalmological examination: Initial baseline and regular ongoing visual assessment are necessary. (Strong recommendation)
2- Management of the child with BDMH (CP) through multidisciplinary team approach:
◽ Phoniatric role:
1- Management of language, speech, and communication difficulties: through language and speech therapies that are tailored according to the child’s deficits.
2- Management of feeding and swallowing problems and saliva control: after selection of the appropriate therapy option.
◽ Management of co-morbidities by other team members e.g. neurologist, audiologist, physical therapist, etc. (Strong recommendation)
Phoniatrics Late Language Emergence / Language Delay Language Disorders / Autism Spectrum Disorder
“last update: 10 June 2024” Download Guideline
– Executive Summary
The scope of the guideline is the diagnosis, assessment and intervention of communication difficulties in children with late language emergence or autism spectrum disorder.
Late Language Emergence
▪️ When a child is first referred for a delay in his/her language development, a detailed thorough history taking should be carried out in order to learn more about the child’s perinatal, developmental, medical, behavioral, social and educational history and to double check the possible existence of any comorbid disorders and/or associated syndromes (Strong recommendation).
▪️ Based on the information gathered during the initial parent interview, necessary referrals are recommended such as audiological assessment (mandatory), neurological examination, physical therapy examination (based on concerns raised by caregivers or deduced during professional observation), special tests related to Autism spectrum disorder (if related features have been reported during the initial parent interview or clinically observed), occupational therapy (if motor programming and/or sensory issues are suspected), etc. (Strong recommendation)
▪️ Following the initial interview, the evaluation process takes place. (Strong recommendation).
▪️ Assessment can be preceded by a screening process (Conditional recommendation).
▪️ A thorough assessment is recommended in order to closely inspect the child’s language skills and establish a proper baseline for future realistic as well as effective therapeutic plans (Strong recommendation).
▪️ Differential diagnosis along with interpretation of all findings and sharing results within the family need to follow the assessment (Strong recommendation).
▪️ Following the evaluation phase, the child is referred for intervention. Intervention can be in the form of indirect intervention; carried out through a series of systematic parent counseling sessions that involves close observation to the child’s skills. This is usually recommended for very young children. For older children, direct intervention takes place (Strong recommendation).
▪️ Direction intervention procedures and strategies can vary depending on the child’s needs, developmental level, family circumstances and other factors. It can be in the form of regular individual therapeutic sessions, group therapy, tasks during naturalistic settings, or a hybrid approach involving a mixture of various direct and indirect approaches all together (Strong recommendation).
▪️ Family involvement is very important in every step as it can help foster, maintain and generalize language skills acquired during formal therapeutic settings and facilitate their generalization to daily life activities and interactions (Strong recommendation).
▪️ Multidisciplinary team involvement is important whenever needed (Strong recommendation).
▪️ In severe case, augmented communication needs to be considered along with working on enhancing spoken language skills (Strong recommendation).
▪️ Equally important to family involvement, is regular data collection for the child’s response to therapy and his/her benefit from selected objectives (Strong recommendation).
Autism Spectrum Disorder (ASD)
▪️ Dealing with a child suspected to be on the Autism Spectrum Disorder (ASD) follows the same management steps mentioned above but with particular focus on collecting additional data and carrying out further testing in order to confirm or exclude the existence of the warning signs of this disorder in addition to particular stress on the child’s social communication skills (Strong recommendatio
▪️ Following initial interview, the child’s eye gaze, joint attention, social interactions, imitation skills, non-verbal means of communication, language skills, facial expressions, repetitive movements, etc. are thoroughly screened and closely observed (Strong recommendation).
▪️ Screening can be followed by a formal testing for cooperative children in order to reach a better understanding of the child’s needs and difficulties (Conditional recommendation).
▪️ The assessment process should also include input from other professionals involved in the inter/multi-disciplinary team dealing with the child (Conditional recommendation).
▪️ If a diagnosis of ASD is proven, relevant therapeutic procedures should immediately follow (Strong recommendation).
▪️ Based on the assessment findings, therapy is provided (Strong recommendation).
▪️ In ASD children, management usually occurs within the frame of a multidisciplinary approach; with all professionals involved collaborating together in order to confirm / exclude the preliminary diagnosis given, plan future therapy, provide support to parents and work towards achieving future targeted goals (Conditional recommendation).
▪️ It is essential that all the professionals involved in the multidisciplinary team possess knowledge of typical and atypical patterns of development in the domains of cognition; communication; emergent literacy; and motor, sensory, and social-emotional and work collaboratively together (Strong recommendation)
▪️ Intervention can vary based on the severity of the disorder and associated problems. Treatment can include activity schedules, visual support aids, or even augmentative and alternative communication (to be used in an augmentative rather than alternative method; i.e., always linked to a verbal message) (Strong recommendation).
▪️ Among the intervention procedures in such cases are also different behavioral intervention techniques and cognitive behavioral therapy (Conditional recommendation).
▪️ Therapy can also include spoken language intervention, parent-mediated intervention, applied behavior analysis, and social-communication intervention (Strong recommendation).
▪️ Socio-pragmatic skills are crucial to address during every stage in the intervention process. Pragmatic skills are usually an area of particular need for patients having Autism Spectrum Disorder (Strong recommendation).
▪️ Transitioning with youth and adults is also very important to consider when children get older in order to help them face high social demands, overcome communication challenges, and better cope with colleagues and peers in all educational as well as vocational and social settings (Conditional recommendation).
Monitoring progress achieved in every stage, not only in structured therapeutic sessions but also during various daily life activities and interactions, can help in consistently updating the child’s therapeutic plan; based on achieved progress and in the highlight of his capabilities; thereby helping him reach the best utmost level; each within his own learning potential (Strong recommendation).
PHONIATRICS Learning disability CORRECTED
“last update: 10 June 2024” Download Guideline
– Executive Summary
Common red flags for learning disabilities: • Discrepancy between child’s ability versus his/her academic achievement. • Phonological awareness problem. • Sound production difficulty. • Syntactic errors. • Word finding difficulty. • Reading comprehension problems(Strong recommendation).
First step in assessment is to exclude other factors that might account for academic underachievement, such as: • Hearing impairment • Visual impairment (uncorrected errors) • Intellectual disabilities • Neurodevelopmental disorders • Environmental factors (e.g. inappropriate educational instruction) • Insufficient motivation (Strong recommendation).
Through psychometric evaluation (IQ assessment), the child is put in one of the following 3 categories: A. Specific learning disability (SLD) (if IQ≥ 85). These children will be subjected to SLD training program. B. Slow learner (if IQ 70-84). These children are candidates for “integration” and should receive same SLD training program except for phonological awareness training. C. Intellectual disability (if IQ < 70). These children need special schools and special education(Strong recommendation).
When the diagnosis of SLD is established, the following assessments should be undertaken: • Assessment of comorbidities: including central auditory processing disorders (CAPD) through special tests, and attention deficit hyperactivity disorder (ADHD) through Conner’s test. • Assessments to delineate the areas of deficit, such as: Language test, psycholinguistic abilities test, dyslexia test, reading test, phonological awareness (PA) test, dysgraphia disability scale (Strong recommendation).
Management of SLD depends on its type as follows: a) Management of dyslexia includes: • Phonological awareness training. • Phoneme/grapheme correspondence & alphabetic reading therapy. • Automatic decoding therapy. • Interventions for reading comprehension. b) Management of dysgraphia is based on its type whether dyslexic, motoric, or spatial dysgraphia. Management of dyscalculia through specific mathematics strategies (Strong recommendation).
Post stroke Oropharyngeal dysphagia
“last update: 28 April 2024” Download Guideline
– Executive Summary
The Phoniatrician’s role is:
- Identifying signs and symptoms of dysphagia;
- Identifying normal and abnormal swallowing anatomy and physiology supported by imaging;
- Identifying indications and contraindications specific to each patient for various assessment procedures;
- Identifying signs of potential disorders in the upper aerodigestive and/or digestive tracts and making referrals to appropriate medical personnel;
- Assessing swallow function as well as analyzing and integrating information from such assessments collaboratively with medical professionals, as appropriate;
- Providing treatment for swallowing disorders, documenting progress, adapting and adjusting treatment plans based on patient performance
- Identifying and using appropriate functional outcome measures;
- Understanding a variety of medical diagnoses and their potential impact(s) on swallowing;
- Recognizing possible contraindications to clinical decisions and/or treatment;
- Being aware of typical age-related changes in swallow function;
- Providing education and counseling to individuals and caregivers;
- Respecting issues related to quality of life for individuals and/or caregivers;
- Practicing interprofessional collaboration;
- Advocating for services for individuals with swallowing and feeding disorders;
- Determining the effectiveness and possible impact of current diet on overall health (e.g., positioning, feeding dependency, environment, diet modification, compensations).
➡️Purpose
Appraisal of the research evidence that exists to support the use of instrumental measures in the clinical assessment of patients with PSOPD. And outline the measures used in its management.
Specifically, the goals are to improve diagnostic accuracy, identify post stroke cases who are most susceptible to OPD, and educate clinicians regarding assessment and rehabilitation
➡️The target audience
The guideline is intended for all clinicians who are likely to diagnose and manage OPD
Pure-Tone Air-Conduction and Bone-Conduction Threshold Audiometry with and without Masking in Adults and Older Children (ECPG)
“last update: 26 August 2024” Download Guideline
– Executive Summary
1. Equipment and test environment
• Audiometer, transducers and response buttons SHALL be clean and calibrated. (Strong Recommendation)
• Ambient noise SHOULD NOT exceed the levels permitted (35dB (A)) measured by the sound level meter. (Conditional Recommendation)
• Infection control measures SHOULD be applied. (Conditional Recommendation).
2. Preparation of the test (Strong Recommendation)
• Otoscopic examination: Findings recorded, including the presence of wax and ear canal collapse. Occluding wax SHALL be removed prior to audiometry and use insert earphone in case of ear canal collapse.
• Subject SHALL be asked about any exposure to loud noise during the previous 24h. If the answer is yes, then more details SHOULD be obtained regarding the exposure and results recorded. Temporal threshold shift should be taken into consideration. It may be necessary to re-test the subject at a time when they have had no recent exposure to noise.
• Subjects SHALL be asked if they have tinnitus, if yes, start with ear without tinnitus and a frequency modulated or warble tone may be used as a stimulus. It is essential to record at which frequencies and in which ears warble tones were used. The use of pulsed tones and narrow-band noise is not advised due to calibration and perception problems.
• Subjects SHALL be asked if they have better hearing in one ear, if so, testing SHOULD commence with that ear.
3. Threshold Estimation (Air/Bone conduction audiometry)
• Instructions: Remove any hearing aids, also any glasses, headwear or earrings that may obstruct the correct placement of the transducers, cause discomfort or affect sound transmission. Wherever possible, hair, scarves etc, SHOULD NOT be allowed to sit between the ear and the transducer. (Conditional Recommendation)
• Subject’s response: SHOULD be clear. (Conditional Recommendation)
Earphones:
There are three main types of transducers that can be used for air-conduction audiometry: supra-aural, circum-aural and insert earphones. (Strong Recommendation)
➡️Test order (Conditional Recommendation)
Start with the better-hearing ear (according to the subject’s account) and at 1000 Hz. Next, test
2000 Hz, 4000 Hz, 8000 Hz, 500 Hz and 250 Hz in that order. Then, for the first ear only, retest at 1000 Hz.
➡️Timing of the test stimuli (Conditional Recommendation)
The duration of the presented tone SHALL be varied between 1 and 3 seconds. The interval between the tones SHALL be varied between 1 second and at least 3 seconds.
➡️Initial familiarization (Conditional Recommendation)
Present a tone of 1000 Hz that is clearly audible (e.g. at 40 dB HL for a normally hearing subject or approximately 30 dB above the estimated threshold for a subject with a hearing impairment, but never more than 80 dB HL). If there is no response, increase in 10-dB steps until a response occurs. If the tone is still inaudible at 80 dB HL, increase 5-dB steps until a response occurs, taking care to monitor the subject for discomfort.
➡️Method for finding threshold. (Conditional Recommendation)
Threshold is defined as the lowest level at which responses occur in at least half of a series of ascending trials with a minimum of two responses required at that level. Apply the method of (Down 10dB up 5dB till 50% response)
+/- masking. Start with 1 KHz. Proceed to the next frequency, starting at a clearly audible level (e.g. 30 dB above the adjacent threshold) in the frequency range 250-8000Hz.
Variations in technique SHALL be recorded (Strong Recommendation)
➡️Bone conduction audiometry
Placed over the mastoid prominence of the worse hearing ear (Strong Recommendation)
Performed in the frequency range 500 Hz to 4000. Tested ear should be occluded with ear plug when testing 4000 Hz b-c. The procedure is similar to the AC audiometry. (Conditional Recommendation)
4. Masking (Conditional Recommendation)
Cross-hearing and masking
• Rule 1
Masking is needed at any frequency where the difference between the left and right not-masked a-c thresholds is 40 dB or more when using supra- or circum-aural earphones or 55 dB when using insert earphones.
• Rule 2
Masking is needed at any frequency where the not- masked b-c threshold is better than the air-conduction threshold of either ear by 10 dB or more.
• Rule 3
• Masking will be needed where the b-c threshold of one ear is more by 40 dB (if supra or circum-aural earphones have been used) or 55 dB or more (if insert earphones have been used) than the not- masked a-c threshold attributed to the other ear.
• Instructions for masking
Procedure for masking (plateau-seeking method for masking)
▪️ Re-establish hearing threshold in the test ear by presenting the tone and seeking the response without masking noise to remind the subject what to listen for.
▪️ Introduce masking noise to the non-test ear. The initial level of masking should be the effective masking level which is equal to the tonal threshold level of that ear at that frequency.
▪️ Using increments of 10 dB in masking noise, until you have at least four measurements (including the initial starting point) and until three successive measurements yield the same tonal threshold. You may be unable to obtain this plateau due to maximum level of the audiometer being reached or because the subject finds the masking noise uncomfortable.
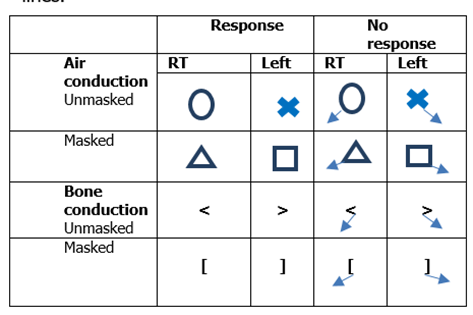
5. Audiometric Description Recommended format and symbols (Conditional Recommendation)
• Five descriptor average hearing thresholds levels (dB HL) according to (ASHA, 2015). These are based on the average of pure tone hearing threshold at frequencies (250Hz, 500 Hz, 1KHz,2 KHz and 4KHz).
|
Mild |
26-40 (Adults)/ 16-40 (Children) |
|
Moderate |
41-55 |
|
Moderately Severe |
56-70 |
|
Severe |
71-90 |
|
Profound |
More than 91 |
Report SHOULD illustrate (Type, Degree and configuration) of the hearing loss. There are three basic types of hearing loss: conductive, sensorineural hearing loss (SNHL), and mixed (ASHA, 2005). The configuration, or shape, of the hearing loss refers to the degree and pattern of hearing loss across frequencies. For example, a hearing loss that only affects the high tones would be described as a high-frequency loss.
• Recommended format and symbols as the following table (ASHA, 1990).
• Air-conduction symbols SHOULD be connected with continuous straight lines; bone-conduction symbols SHOULD be joined with broken lines.
Rehabilitation of Laryngectomised Patients Adapted (ECPG)
“last update: 10 June 2024” Download Guideline
– Executive Summary
1- The patient is presented with severe dysphonia, dysphagia and/ or stridor (conditional recommendation).
2- Patient interview and data collection are needed followed by detailed endoscopic, radiological and laboratory investigations (conditional recommendation).
3- If assessment revealed the presence of extensive malignant laryngeal mass, patient should be informed about the possible lines of intervention, including total laryngectomy (conditional recommendation).
4- Pre-operative assessment of voice and swallowing is done (conditional recommendation).
5- Total laryngectomy decision is taken, based on all pre-operative assessment lines and the surgery is done (strong recommendation).
6- The post-operative anatomical and physiological changes have to be discussed with the patient as well as the expected communication and swallowing problems after intervention (conditional recommendation).
7- Post-intervention detailed assessment is needed (conditional recommendation) including:
▪️ Patient interview and case history.
▪️ Baseline assessments of communication and swallowing are done & instrumental assessments may be needed for evaluation of the oro-pharyngeal swallow using video-Fluoroscopic swallowing Study (VFSS).
▪️ Questionnaires about quality of life may be administered.
8- Then the rehabilitation plan is tailored according to the patient conditions and preferences (strong recommendation):
a. Voice and speech rehabilitation is done by any of the following methods:
▪️ Tracheo-esophageal puncture using speech valve e.g., Provox or Blom & Singer speech valves.
▪️ Esophageal speech (unaided) training sessions
▪️ Electro-larynx or external vibrator.
b. Swallowing and smell rehabilitation may be needed according to the difficulty (conditional recommendation).
c. Care of the neck stoma includes measures of protection against dust, dryness and droplet infection. The use of Heat and Moisture Exchanger (HME) system may help protection of the air way (conditional recommendation).
Tinnitus (ORL) ECPG
“last update: 10 June 2024” Download Guideline
– Executive Summary
Tinnitus is described as ringing, buzzing, clicking, or pulsating noise perceived only by the patient (subjective) or the examiner and the patient’s objective. It may be without aberrant cause (Primary) or due to a specific cause (Secondary) (Strong Recommendation).
Clinicians should perform a targeted history and physical examination at the initial evaluation of a patient with presumed primary tinnitus (Strong Recommendation).
Clinicians must distinguish patients with bothersome tinnitus from patients with no bothersome tinnitus (Strong Recommendation).
Clinicians should distinguish patients with bothersome tinnitus of recent onset from those with persistent symptoms (≥ 6 months) (Strong Recommendation).
Clinicians should obtain a prompt, comprehensive audiological examination in patients with tinnitus that is unilateral, persistent (≥ six months), or associated with hearing difficulties (Strong Recommendation).
Clinicians may obtain an initial comprehensive audiological examination in patients who present with tinnitus (regardless of laterality, duration, or perceived hearing status) (Conditional recommendation).
Clinicians should obtain imaging studies of the head and neck in patients with tinnitus, especially if they have one or more of the following: tinnitus that localises to 1 ear, pulsatile tinnitus, focal neurological abnormalities, or asymmetric hearing loss (Strong Recommendation).
Clinicians should educate patients with persistent, bothersome tinnitus about management strategies (Strong Recommendation).
Clinicians should recommend a hearing aid evaluation for patients with hearing loss and persistent, bothersome tinnitus (Strong Recommendation).
Clinicians may recommend sound therapy to patients with persistent, bothersome tinnitus (Strong Recommendation).
Clinicians should recommend cognitive behavioural therapy to patients with persistent, bothersome tinnitus (Strong Recommendation).
Clinicians can recommend antidepressants, anticonvulsants, or anxiolytics for a primary indication of treating persistent, bothersome tinnitus (Neramexane, Vestipitant alone or in combination with paroxetine, acamprosate, and dietary zinc supplements) (Conditional recommendation).
Clinicians can recommend Ginkgo biloba, melatonin, zinc, or other dietary supplements for treating patients with persistent, bothersome tinnitus (Conditional recommendation).
Clinicians should not prescribe for patients with persistent bothersome tinnitus (Strong Recommendation).
Intratympanic steroids should be used in acute tinnitus, cases with sudden SNHL and cases with SNHL not more than 30 dB, while Intratympanic lidocaine should be tried only for chronic tinnitus (Conditional recommendation).
Surgical treatment is offered for specific causes of tinnitus (e.g. glomus, vestibular schwannoma) (Strong Recommendation).
Tonsillectomy in Children
“last update: 28 April 2024” Download Guideline
– Executive Summary
This guideline predominantly addresses indications for tonsillectomy in children based on obstructive and infectious causes. The evidence that supports tonsillectomy for orthodontic concerns, dysphagia, dysphonia, secondary enuresis, tonsilliths, halitosis, and chronic tonsillitis is limited and generally of lesser quality, and a role for shared decision making is present.
· Clinicians should recommend watchful waiting for recurrent throat infection if there have been<7 episodes in the past year, <5 episodes per year in the past 2 years, or <3 episodes per year in the past 3 years.
· Clinicians should administer a single intraoperative dose of intravenous dexamethasone to children undergoing tonsillectomy.
· Clinicians should recommend ibuprofen, acetaminophen, or both for pain control after tonsillectomy.
· Clinicians should assess the child with recurrent throat infection who does not meet criteria in KAS 2 for modifying factors that may nonetheless favor tonsillectomy, which may include but are not limited to multiple antibiotic allergies/intolerance, PFAPA (periodic fever, aphthous stomatitis, pharyngitis, and adenitis), or history of >1 peritonsillar abscess.
· Clinicians should not order ASOT. The determination of the antistreptolysin-O titer (ASOT) and other streptococcal antibody titers does not have any value in acute and recurrent tonsillitis / pharyngitis.
· Clinicians should ask caregivers of children with obstructive sleep-disordered breathing and tonsillar hypertrophy about comorbid conditions that may improve after tonsillectomy, including growth retardation, poor school performance, enuresis, asthma, and behavioral problems.
· Before performing tonsillectomy, the clinician should refer children with obstructive sleep-disordered breathing for polysomnography if they are <2 years of age or if they exhibit any of the following: obesity, Down syndrome, craniofacial abnormalities, neuromuscular disorders, sickle cell disease, or mucopolysaccharidoses.
· The clinician should advocate for polysomnography prior to tonsillectomy for obstructive sleep-disordered breathing in children without any of the comorbidities listed in KAS 5 for whom the need for tonsillectomy is uncertain or when there is discordance between the physical examination and the reported severity of oSDB.
· Clinicians should recommend tonsillectomy for children with obstructive sleep apnea documented by overnight polysomnography.
· Clinicians should counsel patients and caregivers and explain that obstructive sleep-disordered breathing may persist or recur after tonsillectomy and may require further management.
· The clinician should counsel patients and caregivers regarding the importance of managing posttonsillectomy pain as part of the perioperative education process and should reinforce this counseling at the time of surgery with reminders about the need to anticipate, reassess, and adequately treat pain after surgery.
· Clinicians should arrange for overnight, inpatient monitoring of children after tonsillectomy if they are <3 years old or have severe obstructive sleep apnea (apnea-hypopnea index >10 obstructive events/hour, oxygen saturation nadir <80%, or both).
· Clinicians should follow up with patients and/or caregivers after tonsillectomy and document in the medical record the presence or absence of bleeding within 24 hours of surgery (primary bleeding) and bleeding occurring later than 24 hours after surgery (secondary bleeding).
· The guideline group made a strong recommendation against prescribjng perioperative antibiotics to children undergoing tonsillectomy.
· Clinicians may recommend tonsillectomy for recurrent throat infection with a frequency of at least 7 episodes in the past year, at least 5 episodes per year for 2 years, or at least 3 episodes per year for 3 years with documentation in the medical record for each episode of sore throat and 1 of the following: temperature >38.3 C, cervical adenopathy, tonsillar exudate, or positive test for group A betahemolytic streptococcus
Tympanometry
“last update: 5 August 2024” Download Guideline
– Executive Summary
The tympanometer and probe tip shall be clean (i.e. free from dust and dirt and in compliance with local infection control standards). Tympanometers shall meet the performance and calibration requirements of BS EN 60645–5. (strong recommendation).
Calibration: The calibration of the instrument shall be checked daily with the probe fitted to an appropriate cavity such as the one supplied by the manufacturer. (strong recommendation).
The subject should be seated comfortably and should remain as still as possible during the test. (strong recommendation)
Young children may need to be held by an appropriate adult, which should be the person responsible for the child. (conditional recommendation)
Tympanometry shall be preceded by otoscopic examination to ensure that there are no contraindications to continue. (strong recommendation)
Testing shall proceed only with informed consent (e.g. verbally) from the subject or person responsible for the subject and if it is the judgement of the tester that it is safe to do so. (conditional recommendation)
Subjects with age over 6 months, using a 226-Hz probe tone is recommended (Strong recommendation)
Subjects with a corrected age under 6 months using a 1000-Hz probe tone. (strong recommendation)
Tympanometric results do not identify pathology uniquely and should be interpreted in the context of other information from the complete test battery being conducted and with particular regard to the otoscopic findings and history. (Strong recommendation)
Vestibular Rehabilitation for Peripheral Vestibular Hypofunction
“last update: 9 June 2024” Download Guideline
Executive Summary
Audio-Vestibular medicine physicians prescribe the proper therapy plan that could be performed in collaboration with physiotherapist, Clinicians should offer vestibular rehabilitation to patients with acute or subacute UVH. (Strong recommendation), In acute cases; patient might first take symptomatic treatment to control acute symptoms, anxiety and autonomic complaints to be able to start the VRT. Also Clinicians are (strongly recommended) to offer vestibular rehabilitation to patients with chronic UVH and BVH. Clinicians should not offer saccadic or smooth-pursuit exercises in isolation; as they are not specific exercises for gaze stability to individuals with unilateral or bilateral vestibular hypofunction (strong recommendation). Clinicians may provide targeted exercise techniques to accomplish specific goals appropriate to address identified impairments, activity limitations, and participation restrictions (strong recommendation). Clinicians may prescribe static and dynamic balance exercises and prescribe weekly clinic visits plus a home exercise program of gaze stabilization exercises (strong recommendation). Clinicians should offer supervised vestibular physical therapy in individuals with peripheral UVH and BVH (strong recommendation). Clinicians may use achievement of primary goals, resolution of symptoms, normalized balance and vestibular function, or plateau in progress as reasons for stopping therapy; objective and subjective outcome measures could be used, also Patient’s age and physical capabilities should be considered. (Strong recommendation). Clinicians may evaluate factors that could modify rehabilitation outcomes (strong recommendation). Clinicians should offer vestibular rehabilitation therapy to persons with peripheral vestibular hypofunction with the intention of improving quality of life (Strong recommendation).
Voice disorders
“last update: 28 April 2024” Download Guideline
– Executive Summary
· In the GRBAS Scales, four grades of scale are recommended because of their high reproduction rate and sufficient resolution
· Using the VHI and V-RQOL as patient-reported outcome measures They are, strongly recommended as subjective evaluation tools for voice disorders as they are highly reliable and validated
· Laryngoscopy is an essential tool for visualization of the larynx to diagnose the cause of dysphonia
· Laryngostroboscopy is useful for diagnosis of voice disorders. It is also useful for the diagnosis and monitoring. Laryngostroboscopy was useful for the diagnosis of patients with voice disorders in 27.2% of cases
· Acoustic analysis is useful in objective evaluation of voice disorders, especially for evaluating effectiveness of treatment.
· measurement of voice strength, measurement of pitch, measurement of expiratory flow in phonation, measurement of MPT, measured individually or combined
· clinicians should advocate voice therapy for patients with dysphonia from a cause amenable to voice therapy
· Clinicians should inform patients with dysphonia about control/preventive measures
· Clinicians should document resolution, improvement, or worsened symptoms of dysphonia or change in QOL among patients with dysphonia after treatment or observation.
➡️Purpose
Appraisal of the research evidence that exists to support the use of voice measures in the clinical assessment of patients with voice disorders. And outline the measures used in the management of Functional voice disorders.
Specifically, the goals are to improve diagnostic accuracy, identify cases who are most susceptible to voice disorders, and educate clinicians and patients regarding voice disorders
➡️The target audience
The guideline is intended for all clinicians who are likely to diagnose and manage voice disorders